A diagnosis hiding
in plain sight.
A Morbidity and Mortality case presentation.
Disclosures
Purpose of M&M
Outline
Part 01 / 05
Case
A 65-year-old man with metastatic lung cancer and a malignant pleural effusion.
History — Chief Complaint & HPI
Shortness of breath and chest pain
Onset ~2 weeks of progressive dyspnea and central chest discomfort.
Otherwise negative. Denied hemoptysis, hematemesis, melena, fever, or abdominal pain.
- 65M with metastatic lung adenocarcinoma (liver, bone, brain), HTN, prior PE, and prior malignant pleural effusion s/p thoracentesis.
- Noncompliant with oncologic care. Last seen by oncology 10/2025, no ongoing treatment.
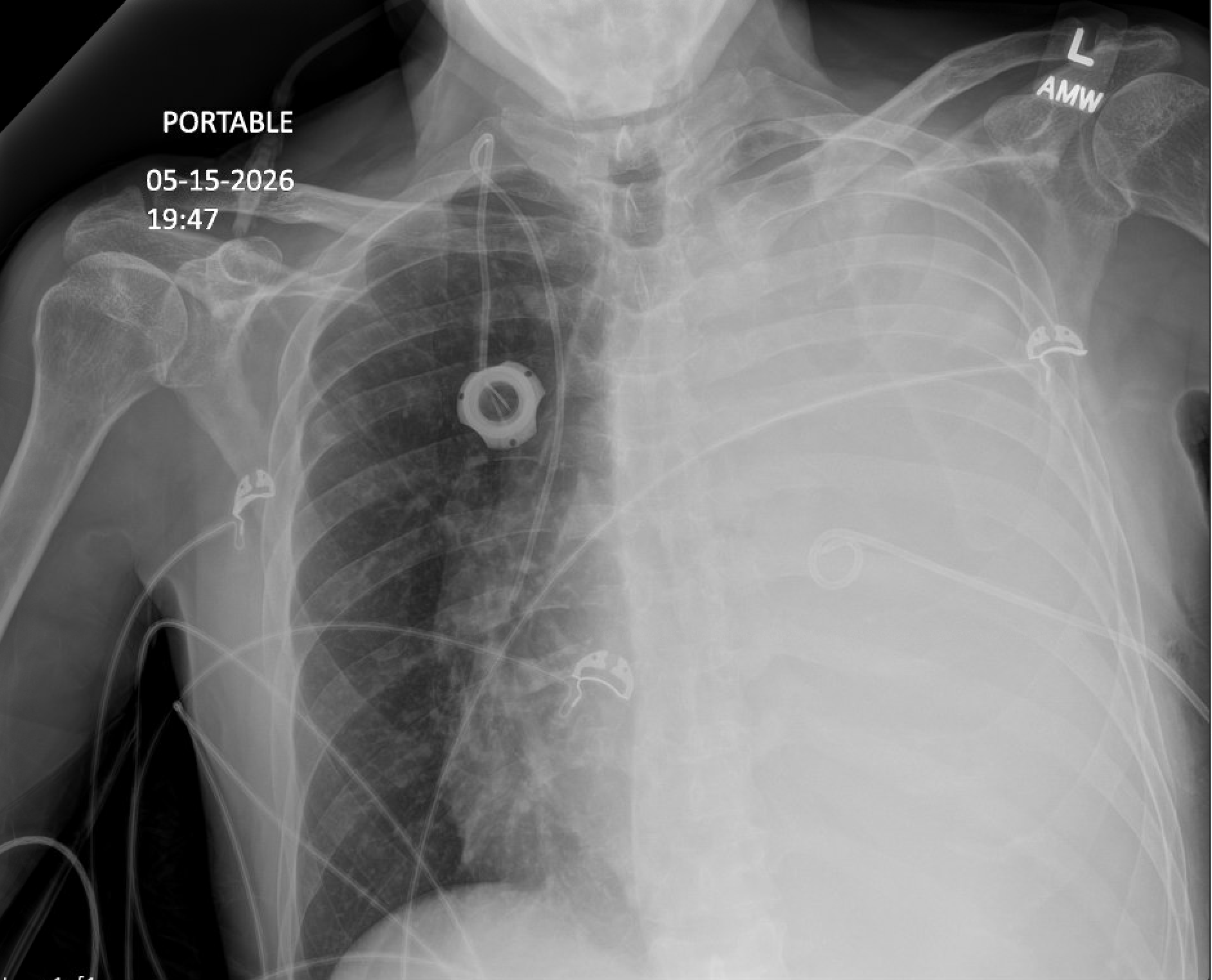
- Presented to ED 5/15/2026 with dyspnea and chest discomfort. CXR showed complete opacification of the left hemithorax.
- CT surgery consulted. Left Fuhrman pigtail chest tube placed in ED, returning bloody pleural fluid (546,897 RBCs). Admitted to IM teaching service.
History — PMH · SH · FH · Medications
- Metastatic lung adenocarcinoma (liver, bone, brain)
- Hypertension
- Prior pulmonary embolism
- Left lower-extremity DVT
- Recurrent malignant pleural effusion s/p thoracentesis
- Lives with his brother
- Former cigarette smoker
- Alcohol / drug use not on file
- Functionally independent at baseline
- Port-A-Cath placement 9/2025
- No other surgical history on file
- Family history non-contributory
- amlodipine, metoprolol (HTN)
- apixaban, self-discontinued 12/2025
- folic acid, ondansetron
- tramadol, hydrocodone–acetaminophen (pain)
Physical Examination
Data — Labs & Studies
- ED chest x-ray: new complete opacification of the left hemithorax, extensive pleural fluid.
- Post-chest-tube CXR (5/15, 19:48): "probable left pleural effusion. No pneumothorax."
- LLE venous Doppler: occlusive DVT, left common femoral to popliteal vein.
- EKG: QTc prolongation.
- SIRS criteria met: tachycardia, tachypnea, WBC 18.2.
Admitting Diagnoses
Initial Management
- Admitted to IM teaching service
- Cardiothoracic surgery + vascular consulted
- Daily chest x-rays obtained with chest tube in place
- Left Fuhrman chest tube placed to suction
- Monitored chest-tube output
- Levalbuterol nebs given
- Empiric vancomycin + piperacillin-tazobactam started
- Blood, urine & pleural cultures obtained
- MRSA nares screen obtained
- Held anticoagulation for bloody effusion and blood-loss anemia
- Serial CBCs, IV fluids, monitored CMP
- Held QT-prolonging meds. Multimodal pain control
Hospital Course — HD 1 to 3
- Admitted. Left Fuhrman chest tube placed in ED for malignant effusion
- Occlusive left LE DVT identified, anticoagulation held (bloody effusion)
- Post-chest-tube CXR: "No pneumothorax"
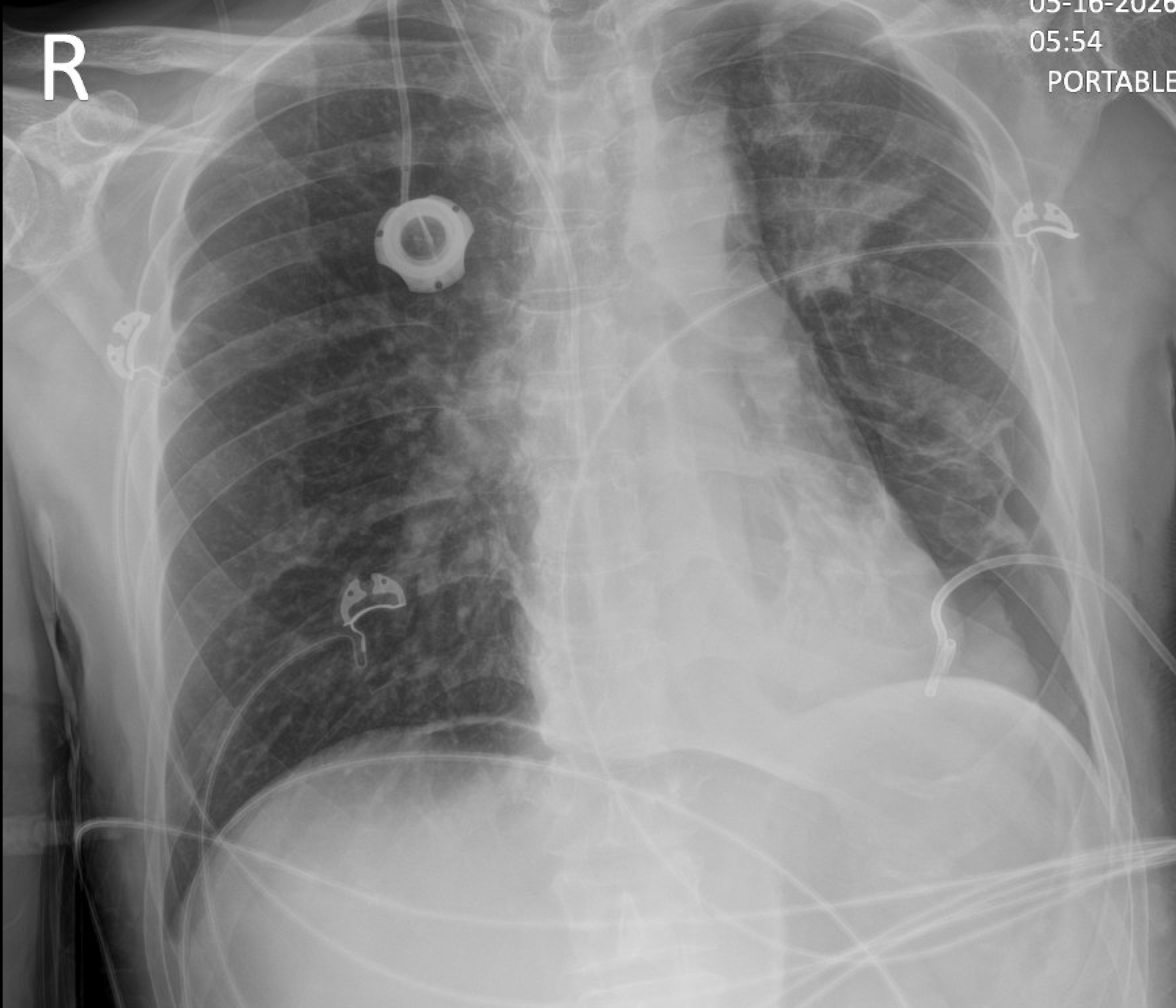
- ~3,700 mL drained, left lung partially re-expands
- Repeat CXR: moderate left hydropneumothorax now present, with a small air leak
- Broad-spectrum antibiotics (vancomycin + Zosyn) continued
- Stable hydropneumothorax, persistent left basilar opacity
- Symptoms improved, dyspnea better, comfortable
- Anticoagulation (apixaban) restarted: 48 h post-tube, Hgb stable
Hospital Course — HD 4 to 5
- Cardiothoracic surgery removes the chest tube (no air leak, lung will not re-expand)
- Radiology calls re: FREE INTRAPERITONEAL AIR on the AM chest x-ray
- Left lateral decubitus film confirms a large pneumoperitoneum
- Patient appears well, sitting up eating breakfast, benign abdomen, no pain
- Read as "low concern for acute process" → serial abdominal exams, CT ordered
- CT abd/pelvis: perforated duodenal ulcer with free air, suspected malignant etiology
- General surgery consulted for perforated viscus
- To OR: exploratory laparotomy, antrectomy + retrocolic gastrojejunostomy, Graham patch
- Large wide-mouth duodenal perforation. EBL 25 mL. NG tube + JP drain placed
Part 02 / 05
Imaging Review
A serial review of the imaging during the hospital course.
Serial Chest Radiographs — HD 1 & 2 · 5/15 → 5/16
Serial Chest Radiographs — HD 3 & 4 · 5/17 → 5/18


5/18 — The Finding That Was Called
PORTABLE · 05-18-2026
- Crescentic lucency outlining both hemidiaphragms, indicating free intraperitoneal air.
- Persistent moderate left hydropneumothorax above it.
- Radiology read: "abnormal upper-abdominal appearance suggests free intraperitoneal air," confirmed on left lateral decubitus.
This is the film that triggered the surgical work-up, on hospital day 4.
CT Confirmation — Hospital Day 5
 CT ABD/PELVIS · 05-19-2026
Cine · 103
CT ABD/PELVIS · 05-19-2026
Cine · 103
Perforated duodenal ulcer of high concern, with new free air and free fluid in the upper abdomen. General surgery consult recommended now.
- Free air and free fluid concentrated in the upper abdomen, with gas tracking along the falciform ligament.
- Fat stranding around the duodenal bulb, plus an abnormal pattern at the peripyloric region with adjacent gas.
- Inflammatory change in the gallbladder, felt to be secondary to the active process.
- Left hydropneumothorax with partial LLL collapse. Known hepatic metastasis (5.4 cm) and right iliac/sacral lesion. Extensive LLE DVT into the left external iliac vein.
Documented at scan: patient reported no abdominal pain. The benign exam persisted to the moment of diagnosis.
Post-operative Course & Outcome
- Confusion overnight requiring soft restraints to protect the NG tube and JP drain
- WBC 26.4 (from 18.5), H/H stable. Started on TPN, NPO, IV antibiotics
- Surgeon: high risk. Desmoplastic reaction suspicious for malignant, non-healing ulcer. Best case a controlled fistula
- Prolonged complex post-operative course on the surgical service
- Transferred out of the unit 6/3 and discharged 6/5
The morbidity under review: a ~2–3 day interval between when free air was retrospectively visible and when the perforation was recognized and repaired.
Part 03 / 05
Discussion
Pneumoperitoneum, the evidence, and where recognition slipped.
Spotlight — Perforated Peptic Ulcer
- Free intraperitoneal air = perforated viscus until proven otherwise.
- The upright chest radiograph is the most sensitive plain film for free air, detecting as little as 1–2 mL beneath the hemidiaphragm.
- But free air is seen in only ~70% of perforated gastric/duodenal ulcers, since many seal quickly. A normal film does not exclude perforation.
- CT is the confirmatory test (sensitivity >95%) and localizes the perforation.
increased risk of death for every hour of delay to source control in perforated peptic ulcer.
- Surgical delay is an independent predictor of mortality.
- Delay beyond 24 h raises mortality several-fold versus ≤6 h.
Perforated Peptic Ulcer — Burden & Lethality
- Perforation is the most lethal complication of peptic ulcer disease, outpacing bleeding in case-fatality.
- Incidence has held steady for decades while the affected population grows older and more comorbid.
- Free perforation produces chemical then bacterial peritonitis → sepsis and rapid physiologic decline.
- Advanced age and major comorbidity. Here, active metastatic malignancy.
- Physiologic derangement at presentation (shock, leukocytosis, hypoalbuminemia).
- Delay from perforation to source control, the single most modifiable factor.
Our patient carried several baseline risk multipliers before any delay, which raised the stakes of every hour.
Risk Stratification — The Boey Score
Mortality climbs stepwise from a score of 0 to 3. Beyond Boey, active cancer, older age and hypoalbuminemia independently predict death. This patient was high-risk on physiology alone, before recognition delay was added.
Free Air on Imaging — Detection Sensitivity
A normal film never excludes perforation. Small free air on a supine portable study, as taken here, is easily missed. Technique (upright/decubitus, 5–10 min positioning) and a low threshold for CT are what close the gap.
When Did the Free Air First Appear?
Management Critique — Guiding Questions
Part 04 / 05
Analysis
Contributing factors & cognitive bias.
Contributing Factors
Swiss Cheese Model — How the Layers Aligned
No single failure, but every defensive layer had a hole on the same day, and they lined up.
Safety Event Classification
Safety Event Reaches the patient and results in moderate-to-severe harm or death.
Safety Event Reaches the patient but causes minimal or no detectable harm.
Safety Event Does not reach the patient. Caught by a barrier or by chance.
A deviation from generally accepted performance standards (GAPS), graded by how far it travelled and the harm it caused.
Classifying This Event
Safety Event The deviation reached the patient and delayed care, but the dominant morbidity was driven by the underlying perforation and metastatic disease. A near-miss for serious harm. Reviewed for learning, not blame.
Part 05 / 05
Matrix & Action Plan
Mapping the case to the healthcare matrix, and a SMART action plan.
The Healthcare Matrix
A framework that maps the case against the IOM's six aims for quality (columns) and the six ACGME core competencies (rows), turning a single case into structured, system-level learning.
Bingham JW, et al. Jt Comm J Qual Patient Saf. 2005;31(2):98–105.
The Case, Mapped — Competencies × Aims
Safe Avoiding injury from care |
Timely Reducing harmful delays |
Effective Evidence-based care |
Efficient Avoiding waste |
Equitable Care that does not vary |
Patient-Centered Respecting preferences |
|
|---|---|---|---|---|---|---|
Patient Care What did we do? |
Anchoring on chest pathology delayed recognition of free air. |
~2–3 days from first visible free air to diagnosis. |
Prompt CT confirmation & operative repair once recognized. |
|||
Medical Knowledge What must we know? |
Read the sub-diaphragm & lung bases on every chest film. |
Post-tube hydropneumothorax ≠ free air. Know film sensitivities. |
||||
Interpersonal & Communication What must we say? |
Closed-loop hand-off of critical incidental findings. |
Honest conversation with patient & family about the delay. |
||||
Professionalism How must we behave? |
Plan honored the patient's wish to eat. Open disclosure via M&M. |
|||||
Systems-Based Practice What is the process? |
Define ownership of incidental findings across shared services. |
Standardize escalation for unexplained sub-diaphragmatic lucency. |
||||
Practice-Based Learning How do we improve? |
Audit interval from first abnormal film to surgical consult. |
Teach systematic film review. Name anchoring and search-satisfaction bias. |
Rows: ACGME core competencies · Columns: IOM aims for improvement. Flagged cells mark where this case fell short.
Patient Care
Medical Knowledge
Systems-Based Practice
Professionalism
Practice-Based Learning
Action Plan — SMART
Summary — Take-Home Points
References
Thank you.
Discussion welcome
